Precision Radiosurgery: Non-Surgical Breakthrough in Managing Complex Brain Metastases

Images showing the Stereotactic Radiation Therapy plan which precisely targets several tumors in the brain with sparing of the normal brain.
The management of brain metastases has undergone a profound transformation in recent years, driven by advancements in radiation oncology that allow for highly precise, targeted therapies. A recent case overseen by Jekwon “Jay” Yeh, MD, Medical Director of Radiation Oncology and Cancer Services at Adventist Health Glendale, and Vice Chairman of the Adventist Health System Radiation Oncology Council, illustrates the impact of radiosurgery when surgical resection is neither feasible nor safe.
Jekwon “Jay” Yeh, MD
The patient, a 77-year-old woman with a history of cervical squamous cell carcinoma treated several years prior, presented in the Emergency Department with acute left-sided weakness. Initially transferred to Adventist Health Glendale under a comprehensive stroke protocol, neuroimaging quickly revealed the true cause: multiple right-sided intracranial lesions consistent with metastatic disease.
Given the deep location of the tumors, Dr. Yeh and neurosurgical colleagues determined that surgical resection carried unacceptably high risks, including significant neurologic morbidity.
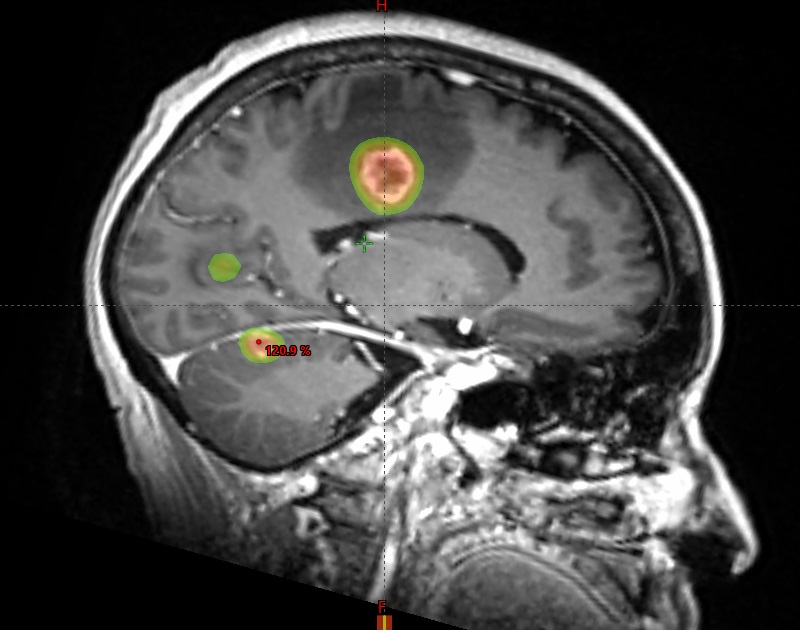
Images showing the Stereotactic Radiation Therapy plan which precisely targets several tumors in the brain with sparing of the normal brain.
This scenario presented a clear therapeutic challenge — how to address symptomatic, unresectable brain metastases in a patient with declining function but preserved systemic health.
According to Dr. Yeh, the case represents the importance of a multidisciplinary approach. When neurosurgical input confirmed the limitations of operative management, radiation oncology was able to offer a precision-based alternative – stereotactic radiosurgery (SRS).
SRS therapy is a minimally invasive surgical intervention that makes use of advanced 3D imaging to deliver highly focused beams of radiation to a specific target, such as a tumor.
Using SRS, Dr. Yeh and his team designed a treatment plan delivering focused, high-dose radiation to each lesion while sparing the surrounding healthy brain tissue.
“Two decades ago, this patient would likely have been offered whole-brain radiation therapy,” notes Dr. Yeh. “Although effective at palliation, whole-brain therapy frequently resulted in neurocognitive decline, hormonal dysregulation, and substantial impact on quality of life. With contemporary radiosurgery techniques, we can achieve tumor control with a fraction of the toxicity.”
Treatment and Response
The patient underwent CT-based simulation, target contouring, and treatment planning within days of admission. She underwent a course SRS treatment. Remarkably, after just two treatments, she reported improved motor function, regaining partial mobility in her left upper extremity. By completion of therapy, she was ambulating with a walker, and at her two-week follow-up, she was walking independently without assistance.
Equally notable was the absence of significant adverse effects. Aside from transient headaches, she experienced no seizures, nausea, or cognitive decline. The rapid functional recovery underscored the radiosensitivity of her lesions and validated the decision to proceed with targeted therapy over more invasive approaches.
Takeaways
The case reinforces several principles relevant to physicians managing patients at risk for or presenting with brain metastases:
- Collaboration is essential. Early involvement of both neurosurgery and radiation oncology ensures that all viable options are considered.
- Radiosurgery offers a safe alternative. For patients with surgically inaccessible tumors, SRS provides local control with minimal morbidity.
- Symptom reversal is possible. Even in cases where corticosteroids (e.g., dexamethasone) fail to provide neurologic relief, radiosurgery may restore function.
- Close surveillance is critical. Post-treatment, Dr. Yeh recommends MRI every three months to detect new lesions early and intervene as necessary.
The evolution of SRS therapy represents one of the most meaningful advances in the management of brain metastases in recent decades. By harnessing this precision technology, physicians can now offer patients functional recovery and disease control without exposing them to the risks of invasive surgery or the neurocognitive decline associated with whole-brain radiation.
For referring physicians, this case serves as a reminder that innovative, non-surgical interventions are available at Adventist Health Glendale — transforming complex, high-risk diagnoses into opportunities for meaningful recovery and improved quality of life.
Implications for Referring Physicians
This case highlights the importance of timely referral to a center with advanced radiation oncology capabilities. Adventist Health Glendale maintains both the technology and the expertise to deliver radiosurgery in the inpatient setting, allowing urgent cases to be addressed without delay.
Additionally, Adventist Health Glendale’s commitment to whole-person care means patients receive highly specialized treatment, but also comprehensive support from a multidisciplinary cancer services team. For this patient, the experience was compelling enough to transfer her ongoing oncology care to Glendale, despite living nearly an hour away.