Don’t Assume Hemorrhoids: how a rectosigmoid lesion harboring invasive carcinoma was successfully treated endoscopically
A case underscoring risk-stratified screening, symptom vigilance, and referral to advanced endoscopy expertise.
A patient in his early 30s came to Dr. James Tabibian, Director of Adventist Health’s Advanced GI Program, with a question many clinicians are hearing more often: “Am I too young to need a colonoscopy?” Having two first-degree relatives with early-onset colorectal cancer, he wasn’t too young — he was high risk.

James Tabibian, MD
“In addition to his family history, the patient also reported intermittent rectal bleeding, further lowering the threshold for colonoscopy,” explained Dr. Tabibian. “More and more, and especially in a case like this, we can’t confidently attribute rectal bleeding to hemorrhoids, even among young adults.”
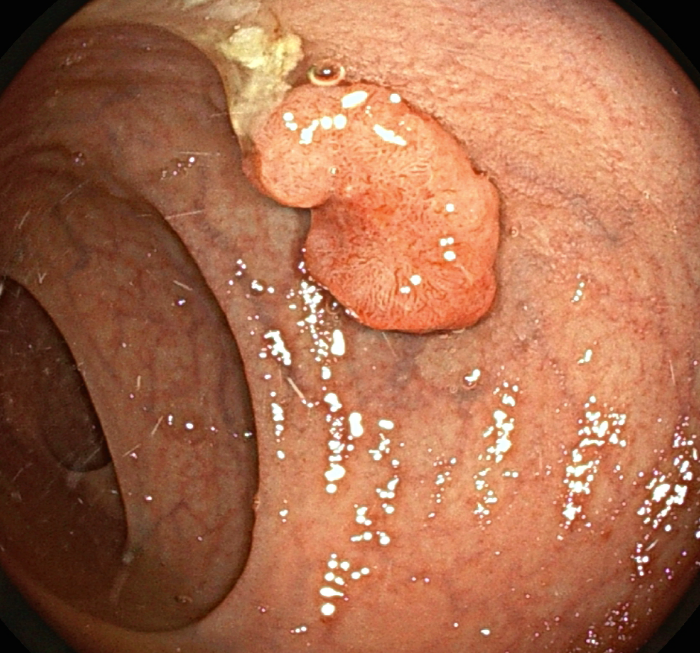
Colonoscopic image demonstrating a polypoid lesion with irregular edges, lobulated surface texture, and focal central depression.
On colonoscopy, the expected finding was there — moderate size internal hemorrhoids. But it wasn’t the finding that mattered most. In the rectosigmoid, Dr. Tabibian identified an approximately 1 cm polypoid lesion that, despite its modest size, carried visual features that raised concern for advanced neoplasia, high-grade dysplasia, and possible carcinoma.
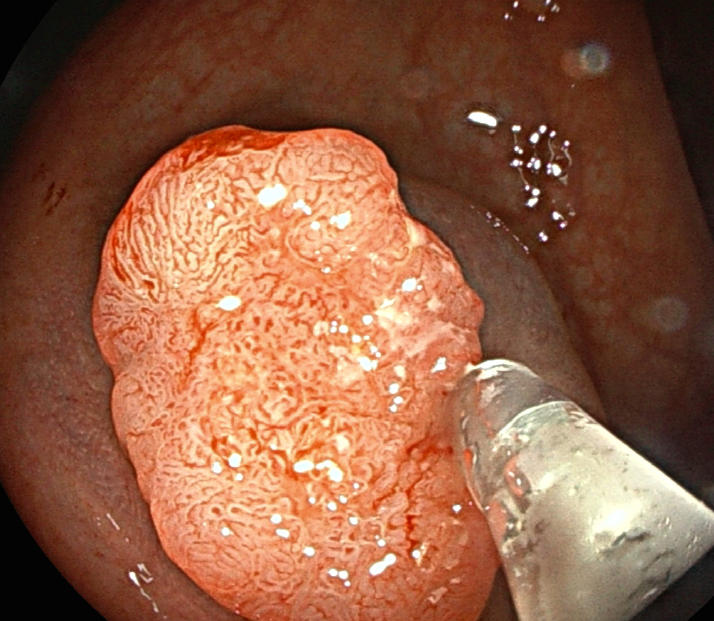
Initial step of submucosal injection to delineate and lift lesion in preparation for endoscopic resection.
In other words: a lesion easy to underestimate and easy to inadequately remove.
Because early cancers and high-risk lesions can be clinically unforgiving to “routine” techniques, the team pursued an approach designed to prioritize real-time oncologic precision. Rather than standard polypectomy or biopsies, the lesion was managed by advanced endoscopic resection methodology— the type of work increasingly central to Adventist Health’s expanding GI footprint across Southern California.
The GI team proceeded directly to hybrid EMR-SD, a technique that leverages the efficiency of endoscopic mucosal resection (EMR) with the depth of endoscopic submucosal dissection (ESD). “The intent was to achieve ample lateral and deep margins and perform en bloc, in toto resection. We believed this was accomplished, and the resection site was closed using through-the-scope clips to reduce the risk of delayed hemorrhage or deep thermal injury,” said Dr. Tabibian. “Histopathology subsequently confirmed invasive carcinoma arising within the lesion. The lateral and deep margins were negative for tumor, and there was no lymphovascular invasion.”
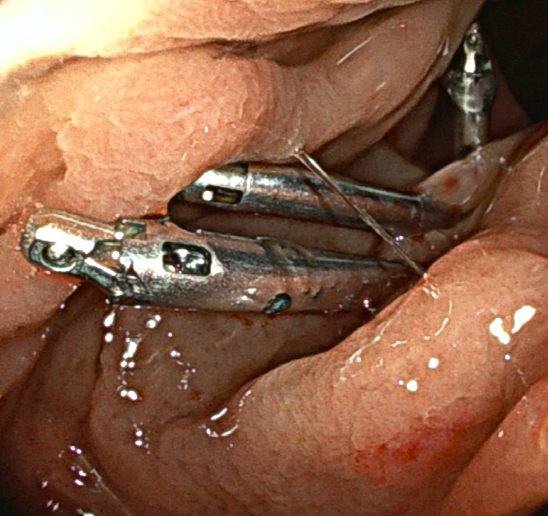
Through-the-scope endoscopic clips used to seal and secure the completed endoscopic resection site
That single finding reframed the entire case: invasive carcinoma — managed endoscopically, with negative margins, avoiding escalation to colectomy and adjuvant therapy. The patient went home that same day and provided counseling regarding the need for close surveillance as a “colon polyp former/cancer former” and the importance of ensuring that first-degree relatives pursue appropriate high-risk screening.
Three practical takeaways for referring clinicians:
- Family history and other risk factors may justify colonoscopy well before age 45 (and uncertainty about timing is reason enough to refer to a gastroenterologist).
- Minor rectal bleeding warrants appropriate workup— avoid anchoring on hemorrhoids, especially in the setting of symptoms or a history potentially pointing to a more sinister etiology.
- Suspicious lesions (even small ones) seen on colonoscopy often benefit from advanced endoscopy expertise, since what is done to a lesion “the first time” can determine short- and long-term options and outcomes.
As Adventist Health’s GI Program continues to grow, supporting patients and referring partners throughout Southern California, our focus is simple: earlier detection, more precise endoscopic therapy, and smoother pathways for patients who need advanced intervention.
If you have questions about high-risk screening, complex polypectomy, EMR, other advanced endoscopic techniques, or a patient you’d like evaluated, Dr. Tabibian and the Adventist Health GI experts welcome your call for consult requests and case discussions.